How do you measure up?
Considerable confusion surrounds the precise meaning of the terms overweight, overfat, and obese. Research emphasizes the need to distinguish between these terms to ensure consistency in use and interpretation.
Overweight
The term overweight refers to a person’s body weight that exceeds an average for height (and perhaps age), usually by some standard deviation unit or percentage value. While many people think of excess weight as being primarily fat, that is not always the case, particularly in active males and females at any age.
Mostly, overweight status determines from standard weight-for-height tables. The first weight-for-height tables were established in 1943 by the Metropolitan Life Insurance Company and later revised in 1983. These tables serve as statistical landmarks based on the average ranges of body weight related to height in which men and women age 25-59 years have the lowest mortality rate. They originally were called “desirable” weight tables, but the phrase “ideal weight” gradually became associated with these tables, even though the word “ideal” was not used in the original or updated publications. Weight-for-height tables do not consider specific causes of death or disease status before death (morbidity). Many newer versions of weight-for-height tables recommend different “desirable” weight ranges, with some considering frame size (whatever that means), age, and gender.
Limitations of weight-for-height tables
Most weight-for-height tables have limited value as a standard to evaluate physique status or health because the term “overweight” often infers extra weight consisting primarily of excess body fat. This often is not the case, particularly for physically active men and women at any age. Competitive athletes clearly illustrate this point; many possess high muscularity and exceed the average weight for their sex and height but otherwise possess very little fat compared to their non-active peers. Some larger-sized persons are indeed “overweight,” yet they may fall within a normal range for body fat without need to reduce weight.
In the early 1940s, Navy physician and medical researcher Albert Behnke (1919–90) was first to assess the body composition of 25 professional football players using methods other than weight-for-height tables. When he applied standards based on height and weight, 17 players failed to qualify for military service because their “overweight” status incorrectly indicated excessive fatness. Carefully evaluating each player’s actual body fat indicated their excess weight consisted primarily of muscle weight, not fat weight. These observations clearly indicate the term “overweight” refers only to body weight greater than some standard, usually the average body mass for a given stature. Being above some “average,” “ideal,” or “desirable” body weight based on weight-for-height tables should not dictate whether someone should reduce weight. A more desirable strategy, particularly for physically active individuals, evaluates body composition (percent body fat, fat weight, and fat-free body weight) by more sophisticated techniques that I will discuss in a future column.
The Body Mass Index: A better use for weight and height
Clinicians and researchers use the body mass index (BMI), derived from body weight related to height squared—Wt ÷ (Ht x Ht)—to evaluate the normalcy of body size. The BMI attempts to be a better indicator of weight status, relative to height, than body weight alone.
The BMI was derived in 1832 by the Belgian mathematician, astronomer, and statistician Adolphe Quetelet (1796–1874). In 1972 Ancel B. Keys (1904–2004), a famous American scientist who was one of the first to study the influence of diet on health status, first used the term “body mass index” to refer to the Quetelet Index, which he thought of as a possible proxy for body fat percentage.
Current classification standards for overweight and obesity (discussed in the next section) assume the relationship between BMI and percentage body fat remains independent of age, gender, ethnicity, and race. For example, Asians have greater body fat content than Caucasians at a given BMI level and thus show greater risk for the fat-related illnesses of obesity and type 2 diabetes. Hispanic-American women also have a higher body fat percentage at a given BMI than European-American and African-American women.
The importance of the BMI is its curvilinear relationship to all-cause mortality; this means that as BMI increases, so does the risk for cardiovascular complications, including hypertension, stroke, type 2 diabetes, and renal disease.
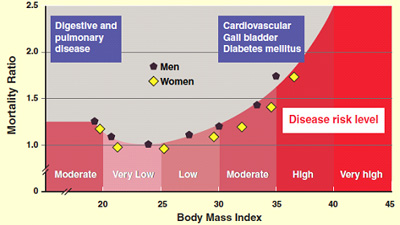
The above figure indicates the level of risk with each 5-unit increase in BMI. The lowest health-risk category occurs for individuals with a BMI between 20-25, whereas the highest risk category includes individuals whose BMI exceeds 40. For women, the desirable BMI ranges between 21.3 and 22.1; the corresponding desirable range for men is 21.9 to 22.4. An increased incidence of high blood pressure, obesity, diabetes, and coronary heart disease occurs when the BMI exceeds 27.3 for women and 27.8 for men. The BMI is expressed in kilograms per meters squared: weight in kilograms ÷ (height in meters X height in meters). Follow the steps below to compute your BMI using weight in pounds and height in inches.
BMI = Weight (kg) ÷ (Height X Height) (m) |
||
| Step 1. Multiply body weight in pounds by 0.4535 to convert to kilograms. | ||
| Step 2. Multiply height in inches by 0.0254 to convert to meters. | ||
| Step 3. Multiply answer in Step 2 by itself to obtain height in square meters (meters squared). | ||
| Step 4. Compute BMI: Divide results of Step 1 by the results of Step 3. |
Overfat
When methods other than height and weight are available to determine human body composition (body-fat weight and fat-free body weight), one can more accurately place an individual’s body-fat level on a continuum from low to high, independent of body weight or height. Overfatness then, refers to a condition in which one’s body fat exceeds an age- and/or gender-appropriate average by a predetermined amount.
Obese
The term obesity refers to the overfat condition that accompanies a constellation of comorbidities that includes one or all of the following components of what is known as the “metabolic syndrome”:
- Glucose intolerance
- Insulin resistance
- Dyslipidemia—high levels of blood fats including triglycerides, LDL-cholesterol, and low levels of HDL-cholesterol
- Type 2 diabetes
- Hypertension
- Increased visceral adipose (i.e., fat) tissue
- Increased coronary heart disease risk
- Increased cancer risk
Research suggests excess body fat, not excess body weight per se, explains the relationship between above-average body weight and disease risk, emphasizing the importance of distinguishing the composition of excess body weight to determine an overweight person’s disease risk. Likewise, many individuals are not overfat but may still exhibit obese correlates.
Caution should be used when using the term obesity, instead of overfatness to describe cases of excess body weight. It is unfortunate that these terms often are used interchangeably without actually measuring body fat and related disease risk. The term obesity with its many pejorative connotations seems unjustified in many instances.
Using BMI to set excess weight and obesity standards
It has become standard practice to use the BMI as a surrogate measure of body fat such that different BMI demarcation values now are used to infer classification status of “normal weight,” “overweight,” and “obese” for health-screening purposes. The fact that BMI positively relates to disease risk, at least in population studies, is used to justify its use in this context, even if it does not relate well to actual body fat estimates for any one individual.
The following BMI-based classification is used to determine the adequacy of one’s body weight. Based on your BMI calculations, what is your classification?
BMI Classifications |
| Normal: ≤25 |
| Overweight: 25-29.9 |
| Obese: ≥30 |
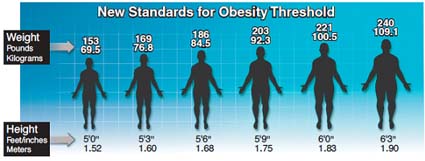
The figure below shows the current standards for identifying obesity (defined by BMI ≥ 30) for six heights (from 5 feet 6 inches tall to 6 feet 3 inches tall). Persons with a BMI of ≥30 average about 30 pounds overweight.
For example, a 6-foot man weighing 221 pounds and a 5-foot-6-inch woman weighing 186 pounds both have a BMI of 30, and both are approximately 30 pounds overweight. The revised standards currently place 65 percent of adult Americans in either the overweight or obese categories—a shocking number—up from 56 percent in just the last 15 years.
Using the BMI standards listed above, the prevalence of childhood and adult obesity has reached epidemic proportions, more than doubling for adults in the United States and globally over the past 30 years. More people are overweight and obese than ever before, a startling statistic by any measure.
Sources:
• American Institute for Cancer Research
• National Heart Lung and Blood Institute
• National Task Force on the Prevention and Treatment of Obesity. Obesity, overweight and health risk. Arch Intern Med 2000;160:898.
• McArdle, W.D.; Katch F.I.; Katch V.L. Sports and Exercise Nutrition, Fourth Edition. (Lippincott Williams & Wilkins, 2013).
• McArdle, W.D.; Katch F.I.; Katch V.L. Exercise Physiology: Nutrition, Energy, and Human Performance, Seventh Edition. (Lippincott Williams & Wilkins, 2010).

Judy Panish
Good Job Brother!! I just did my BMI and I am 22!!!! Loooking good!
Reply