
History lesson
The first diabetes narrative appeared in ancient Egyptian hieroglyphs around 1500 BC, describing a disease characterized by excessive thirst, urination, and weight loss. Similar descriptions appear in ancient Indian, Chinese, and Greek medical texts.
In the 17th century, the English physician Thomas Willis coined the term diabetes mellitus. It derives from the Greek word diabainein, meaning “to pass through” and the word mellitus meaning “sweet” or “honeyed.” The term conveyed the consistently sweet taste of diabetes patients’ urine! In the 18th century, it was discovered that diabetes associated with high blood glucose levels, the main sugar found in blood.
In 1921, researchers Frederick Banting (a Nobel Prize winner from Canada) and Charles Best (an American-Canadian who co-discovered insulin) isolated insulin from a dog’s pancreas. In 1922, the first human patient with diabetes was successfully treated with insulin. Scientists developed synthetic insulin in the 1950s and have made significant advances in diabetes treatment ever since, including the development of insulin analogs, oral antidiabetic drugs, and insulin pumps.
Diabetes in America
In 2024, roughly 38 million people had diabetes, with 1.2 million new cases diagnosed annually. Diabetes and its related complications are the seventh leading cause of death in the U.S. and account for about 25% of total health care costs — about $306.6 billion in direct medical costs, and about $106.3 billion in indirect costs.
Mortality rates from diabetes have been rising since 2000. In contrast, the probability of dying from one of the other three main noncommunicable diseases — cardiovascular diseases, chronic respiratory diseases, and cancer — between the ages of 30-70 has decreased by 20% globally between 2000-19.
Prediabetes is the condition in which blood sugar levels are higher than normal but not high enough for a type 2 diabetes diagnosis. Prediabetes affects 97.6 million adults. More than 1 in 3 American adults have prediabetes, and more than 8 in 10 don’t know they have it.
What is diabetes
Diabetes represents a chronic disease that occurs when either the pancreas fails to produce enough insulin to control circulating blood sugar (Type 1 diabetes – T1D), or when the body cannot effectively use the insulin it produces to facilitate blood sugar entry into muscle cells, (Type 2 diabetes – T2DM).
Type 2 diabetes accounts for about 90-95% of all diagnosed diabetes cases.
Insulin is produced by the pancreas’ beta cells in response to elevated blood sugar (hyperglycemia). Its primary function is facilitating sugar entry into (mostly) muscle cells. The figure below illustrates the insulin response in healthy individuals (left), those with type 1 diabetes (middle), and those with type 2 diabetes (right) in response to elevated blood sugar, like what happens after eating.
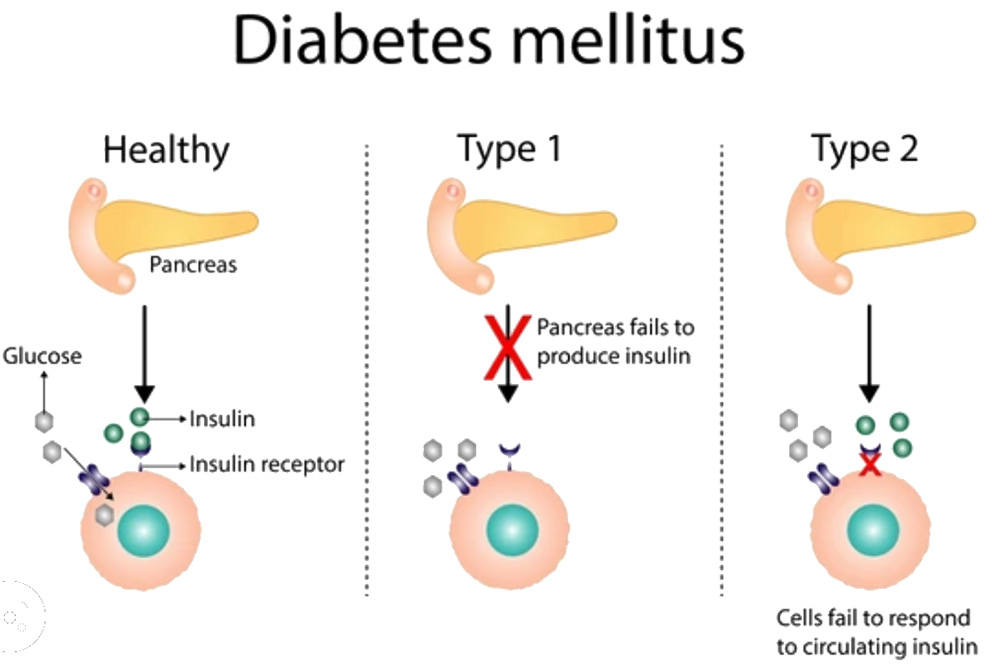
In healthy individuals, insulin acts like a key to unlock insulin receptors on a cell’s surface so they can incorporate the sugar into the cell. When successful, fluctuations of the circulating blood sugar are minimal. In type 1 diabetes, the pancreas fails to produce enough insulin, which results in elevated blood sugar. In type 2 diabetes, insulin receptors become insensitive to the effects of insulin, thus elevating the levels.
Gestational diabetes (GDM)
The percentage of pregnant women with a diagnosis of GDM increased from 6% in 2016 to 8.3% in 2021; in 2023 the percentage ranged from 7%-14%. Each successive maternal age group had more GDM. For mothers aged ≥40 years or older, roughly 15% had GDM, which is nearly six times as high as the rate for mothers aged ≥20 years (2.7%).
How to determine if you have diabetes
Since diabetes represents a disease of unregulated (increased) blood sugar, it can be diagnosed by one of three types of blood tests that measure blood sugar levels.
- Fasting blood sugar test — Measuring blood sugar level after an eight-hour fast. A level of 126 milligrams per deciliter (mg/dL) glucose or higher on two separate tests suggests diabetes.
- Glucose tolerance test — Measuring blood sugar level before and two hours after drinking liquid with a high sugar concentration. A sugar level of 200 mg/dL or higher after two hours suggests diabetes.
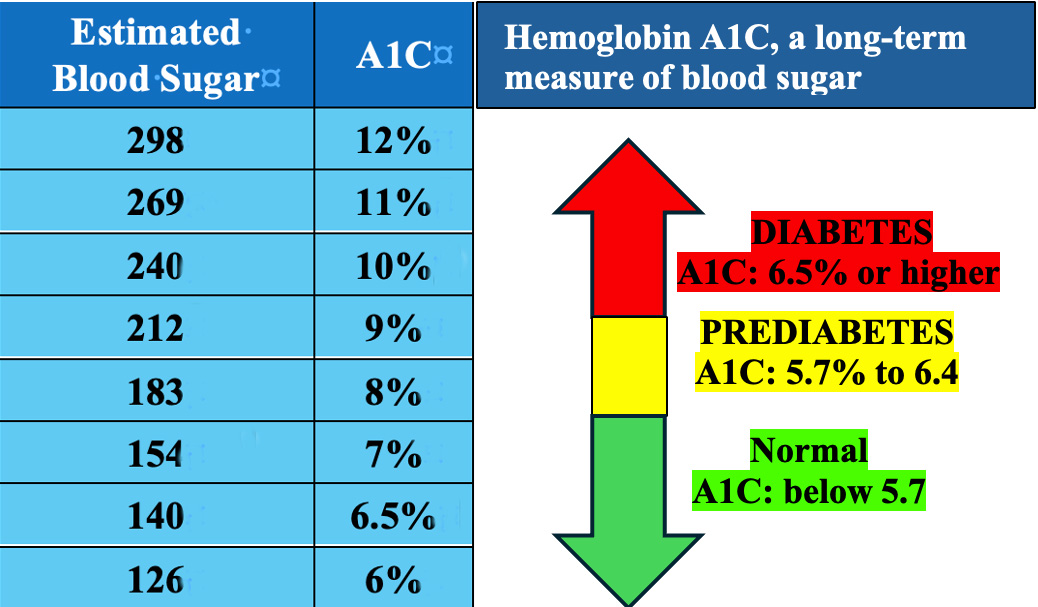
- A1C test (hemoglobin A1C, or HbA1C, or glycated hemoglobin, or glycohemoglobin test) — When blood sugar levels are high, some of it attaches to hemoglobin, a protein in red blood cells. The A1C test measures the percentage of glycated hemoglobin and is representative of the average blood sugar levels over two to three months. The figure below shows the A1C levels and the corresponding blood sugar estimates. A1C levels may vary depending on factors such as age, weight, and medications.
Noninvasive diabetes risk estimate
It is possible to obtain a quick risk estimate for diabetes without a blood test. Below is a general screening test from the American Diabetes Association’s Diabetes Risk Test. If you have a high score, I would urge you to get a blood test for a more definitive blood sugar diagnosis.

Diabetes risk factors
Type 1 diabetes is believed to be caused by an autoimmune reaction (the body attacks itself). There is no known prevention for type 1 diabetes. However, the following risk factors are strong predictors:
- Family history — having a parent, brother, or sister with type 1 diabetes increases risk.
- Age — type 1 diabetes can occur at any age, but usually develops in children, teens, or young adults.
- Caucasian people are more likely to develop type 1 diabetes than African American and Hispanic or Latino people.
Prediabetes and type 2 diabetes
The following are strong predictors if you:
- Are overweight or obese.
- Are 45 years old or older.
- Have a parent or sibling with type 2 diabetes.
- Are physically active less than three times per week.
- Have non-alcoholic fatty liver disease.
- Have ever had gestational diabetes or given birth to a baby who weighed more than 9 pounds.
- Are an African American, Hispanic or Latino, American Indian, or Alaska Native person. Some members of the Pacific Islander and Asian American populations also have a higher risk.
Gestational diabetes
Strong predictors include whether you:
- Had gestational diabetes during a previous pregnancy.
- Have given birth to a baby who weighed more than 9 pounds.
- Are overweight or obese.
- Are age 25 or older.
- Have a family history of type 2 diabetes.
- Have the hormone disorder polycystic ovary syndrome.
- Are an African American, Hispanic or Latino, American Indian, Alaska Native, Native Hawaiian, or Pacific Islander person.
Gestational diabetes usually disappears after giving birth, but having a history of gestational diabetes increases the risk of type 2 diabetes after birth. The baby from a gestational diabetic mother also is more likely to develop obesity as a child or teen, and develop type 2 diabetes later in life.
Diabetes prevention
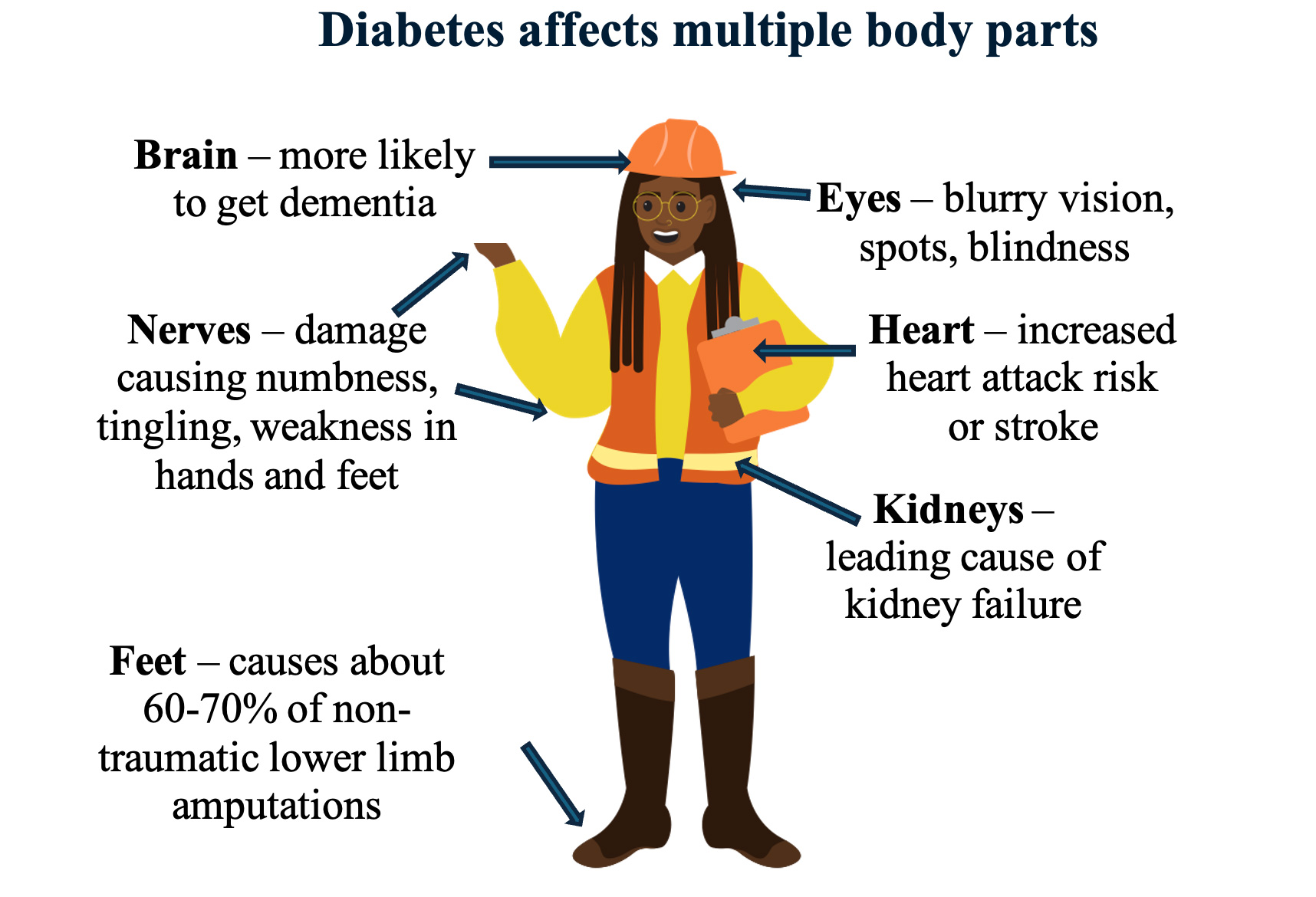
When left untreated, diabetes has far-reaching impacts on the body. (Image: Vic Katch.)
Overwhelming research supports specific lifestyle habits to help prevent or delay type 2 diabetes.
Achieve ideal body weight
A good short-term goal is to lose no more than 1–2 pounds per week.
Physical activity
Aim for at least 150 minutes of moderate to vigorous physical activity (brisk walking, swimming, biking, or running) per week. Include resistance exercise (weightlifting, yoga, or calisthenics) at least 2–3 times a week.
Healthy eating
Choose foods that are lower in calories and reduce foods high in saturated fat and salt. Choose foods that contain healthier fats, such as unsalted nuts, seeds, avocados, olive oil, and sunflower oil. Use whole grains like farro, quinoa, corn, oatmeal, and brown rice instead of refined grains.
Quit smoking
Smoking increases one’s risk of developing type 2 diabetes. There’s no better time or reason to quit!
References
- American Diabetes Association Professional Practice Committee. 8. “Obesity and Weight Management for the Prevention and Treatment of Type 2 Diabetes: Standards of Care in Diabetes-2024.” Diabetes Care 2024;47(Suppl 1):S145-S157.
- Apovian, C.M., et al. Endocrine Society. “Pharmacological management of obesity: An Endocrine Society Clinical Practice Guideline.” The Journal of Clinical Endocrinology & Metabolism 2015;100(2):342.
- Barlas, T., et al. “Credibility of ChatGPT in the assessment of obesity in type 2 diabetes according to the guidelines.” International Journal of Obesity (London) 2024;48(2):271.
- Chait, A., et al. “Lipid-lowering in diabetes: An update.” Atherosclerosis 2024;394:117313.
- Crandall, J.P. et al. “Diabetes Prevention Program Research Group. The prevention of type 2 diabetes.” Nature Clinical Practice Endocrinology & Metabolism 2008;4(7):382.
- Dicken, S.J., et al. “Food consumption by degree of food processing and risk of type 2 diabetes mellitus: A prospective cohort analysis of the European Prospective Investigation into Cancer and Nutrition (EPIC).” The Lancet Regional Health – Europe 2024;(16)46:101043
- Eades, C.E., et al. “Prevalence of gestational diabetes in the United States and Canada: A systematic review and meta-analysis.” BMC Pregnancy Childbirth 2024;24(1):204.
- National diabetes statistics report, 2022. Centers for Disease Control and Prevention. Updated Jan. 18, 2022.
- Prevalence of both diagnosed and undiagnosed diabetes. National diabetes statistics report, 2022. Centers for Disease Control and Prevention. Updated Sept. 30, 2022.

Bill Canning - ‘71&’73
Vic
Great article
Historical beginnings then a no nonsense logical explanation of the disease
Really interesting and well written
Nice job my friend
Bill
Reply