
High five
The leading causes of death and disability in the United States can be traced to five major chronic diseases. Collectively, they are responsible for seven out of every 10 deaths, killing more than 1.7 million Americans each year:
- Heart disease
- Cancer
- Stroke
- Chronic obstructive pulmonary disease
- Diabetes
Chronic diseases are broadly defined as conditions that last one year or longer, require ongoing medical attention, or limit activities of daily living. They are the leading drivers of the country’s annual health-care costs of $4.5 trillion.
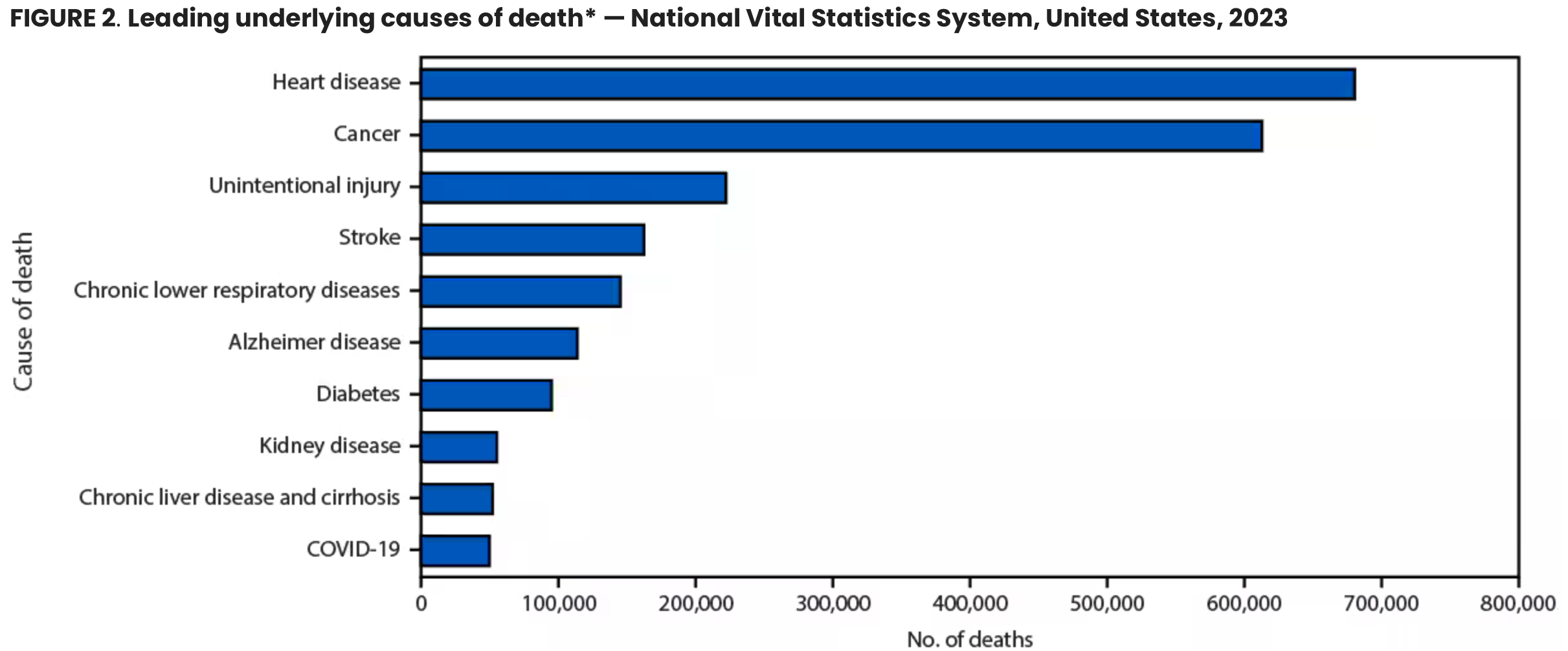
(National Vital Statistics System, 2023. Click on the image to enlarge.)
Comorbidity
Chronic conditions rarely exist in isolation, which complicates the treatment plan. One in four U.S. adults have two or more chronic conditions simultaneously, termed comorbidity. More than half of older adults have three or more chronic diseases. In the U.S., 10,000 or more Americans will turn age 65 each day from now through the end of 2029. It is reasonable to expect that the overall number of individuals with comorbidities will increase. So will the number of deaths caused by chronic diseases.
Causes of chronic disease
Myriad individual and public factors influence a person’s risk of developing a chronic disease. Overall, individual risk factors depend on personal lifestyle choices, including diet and exercise. In contrast, public risk factors tend to be out of one’s own control. The Flint Water Crisis comes to mind. To complicate matters, individual and public chronic disease factors often interact.
Individual risk factors

(Image courtesy of Vic Katch.)
The major individual risk factors for chronic disease are fairly easy to identify:
- Tobacco use
- Dietary factors
- Physical inactivity
- Excessive alcohol consumption
- Elevated blood pressure
- Elevated blood cholesterol
- Elevated blood glucose (sugar)
- Overweight or obesity
- Age
- Gender
- Genetics (family history)
Common wisdom, supported by sufficient scientific evidence, stresses the many benefits of adopting lifestyle changes to reduce the risks of chronic disease. Engaging in regular physical activity and adding more plant-based foods to one’s diet are two of the most common and effective interventions. But such interventions often don’t occur till late adulthood, long after the ravages of poor health practices have allowed the incubation of a chronic disease to reach a critical horizon.
When overt chronic disease symptoms become observable it may be possible to alter disease progression using targeted interventions within any one individual (Health Yourself: Nature v nurture: It’s both). However, these interventions have had little or no effect on a population basis. Chronic disease rates are rapidly rising worldwide, particularly in the more affluent economies. It seems there is little we can do about it: In the U.S., we have failed at every attempt to quell rising cancer, diabetes, hypertension, stroke, heart and respiratory diseases, arthritis, obesity, inflammatory diseases, and oral disease rates.
History of individual risk factors
Efforts to identify individuals at risk for chronic disease are based on early research from the 1950s and 1970s that examined the autopsy reports of soldiers in their 20s, who were killed during the Korean and Vietnam wars. Many exhibited significant atherosclerosis, a narrowing of the coronary artery that associates with later heart attacks. Researchers at the time concluded the soldiers were eating too much fat, smoking cigarettes, and not getting enough exercise. Even though the young soldiers didn’t exhibit overt signs of heart trouble while living, the disease was incubating and likely would have made an appearance years down the road.
This explanation aligns with findings from the noted and ongoing Framingham, Massachusetts Heart Study, which established the importance of individual risk factor development during the early stages of life. The study originally enrolled two-thirds of Framingham’s citizens — 5,209 men and women aged 29-62 — who had not yet developed overt symptoms of cardiovascular disease or suffered a heart attack or stroke. Researchers followed them throughout their lives to see who developed coronary artery disease. The study has now enrolled a third generation of participants. Findings reveal that individuals with high blood pressure, obesity, high cholesterol, and smoking habits were at greatest risk for heart disease and diabetes development.
Encouraging people to stop behaviors associated with disease progression has long been the predominant perspective for population-based health promotion. And it has worked, mostly. In the 1980s, the U.S. Surgeon General and policymakers turned their focus on the tobacco industry, introducing restrictions around production, packaging, advertising, and smoking in public places. Cigarette use declined, along with deaths from heart disease.
Public chronic disease risk factors

(Image courtesy of Vic Katch.)
Some individuals and groups are more susceptible to developing a chronic disease, due to factors that supersede one’s ability to make healthy choices. This points to “public” influences for chronic disease development. Indeed, research suggests that public disease risk factors represent “root causes” for disease development, independent of individual risk factors.
Health epidemiologists study how diseases and other health conditions spread and affect populations, and how to prevent and control them. It’s a key part of public health evidence-based medicine, and is used to shape policy decisions and identify targets for health care. By studying the frequency and pattern of health events in populations, including the number of cases in a given population, epidemiologists can identify environmental, social, genetic, and behavioral factors contributing to chronic disease development.
One of the most cited examples of epidemiology in action was Dr. John Snow’s mapping of the 1854 Broad Street cholera outbreak in London. The “miasma theory” dominated medical thinking at the time: experts believed bad air caused disease. Snow, however, proposed cholera was waterborne. His groundbreaking approach relied on meticulous data collection and analyses. He began by mapping the locations of cholera cases throughout London, a novel method at the time, which allowed him to visualize the spread of the disease. His analyses revealed a pattern of disease spread centered around the Broad Street water pump. Snow conducted interviews with local residents, gathering detailed information on their water sources and daily routines. His methodical approach provided strong empirical evidence that linked the outbreak to the contaminated water supply from the pump.
Economic disparities lead to health disparities
In recent decades, epidemiologists have identified the unequal distribution of wealth, income, and resources in a society as a root cause for health disparities in that society, independent of individual risk factors.
At the most basic level, socioeconomic differences affect access to health care and health outcomes. Epidemiologic analyses of chronic disease development in populations characterized by economic disparity show individuals of lower socioeconomic status suffer higher rates of chronic disease and experience lower life expectancy when compared to those of higher socioeconomic status, in lock-step fashion.
It’s not surprising. Economic disparities create a complex web that ultimately affects individuals’ healthy lifespan. When resources are limited, access to necessary health care, nutritious food, and safe living conditions diminish.
Consequently, individuals from lower socioeconomic backgrounds experience a higher burden of chronic diseases, which can truncate lifespan.
Conclusions
Addressing economic inequality through local, state, and federal policies that increase access to education, living wages, housing, and other resources can help reduce health disparities. Improving the social determinants of health is crucial for reducing chronic disease and promoting more equitable health outcomes.References
- Adogu, Prosper Obunikem Uchechukwu, et al. “Epidemiologic transition of diseases and health-related events in developing countries: A review. The American Journal of the Medical Sciences 2015;5(4):150.
- Ahmadm, F.B., et al. “Mortality in the United States –Provisional data, 2023. The Morbidity and Mortality Weekly Report 2024;73:677.
- Aman, Y. “Addressing gender disparities in global health.” Nature Aging 2024 Jun;4(6):750.
- Amin, S.A., et al. “Disparities and the American health care system.” Clinical Spine Surgery 2019 Mar;32(2):67-70.
- Centers for Disease Control and Prevention. Health Disparities.
- Ezell, J.M. “The health disparities research industrial complex.” Social Science and Medicine 2024;351:116251.
- Hacker, K. “The burden of chronic disease.” Mayo Clinic Proceedings: Innovations, Quality & Outcomes 2024;8(1):112–119.
- Pendyal, A. “Disparities in cardiovascular health: Looking beyond traditional categories.” Canadian Journal of Cardiology 2024;40(6):1176.
- Raghupathi, W., Raghupathi, V. “An empirical study of chronic diseases in the United States: A visual analytics approach.” International Journal of Environmental Research and Public Health 2018 Mar;15(3):431.
- Wamboldt, M.Z. “Introduction to a special section: Racial disparities in health care.” Family Process 2024;63(2):471-474.
- Waters, H., Graf, M., editors. “The costs of chronic disease in the U.S. 1st Ed. Milken Institute“; 2018.
(Lead image: A 3D-rendered, enhanced scanning electron micrograph (SEM) of cancer cells. Source: iStock.)

Dawn Burris
People are unhealthy because we are being systematically poisoned. Maybe that would be a better conversation to have.
Reply